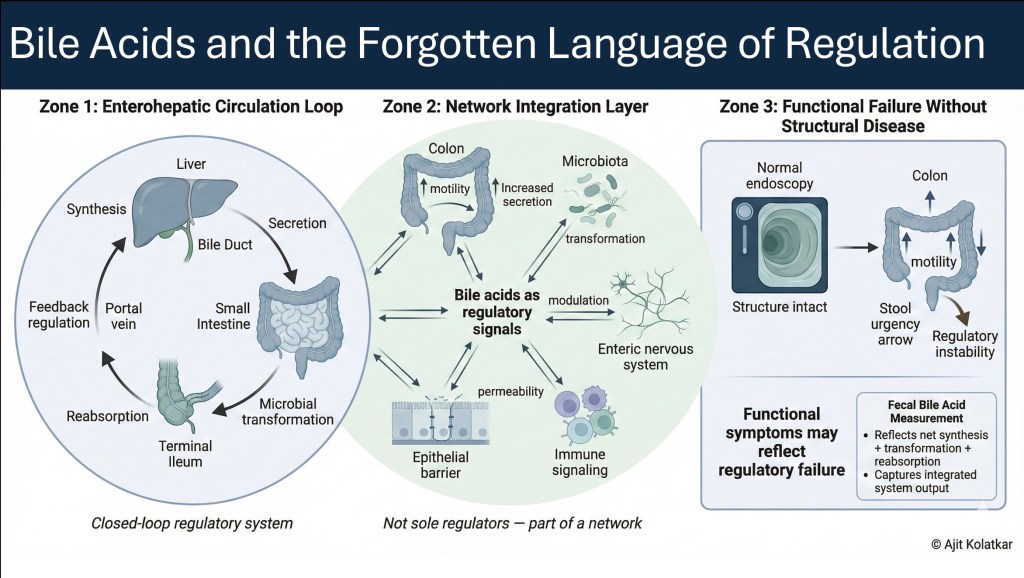
Figure 1 illustrates the critical diagnostic gap between structural integrity and functional failure in gastrointestinal health. While traditional imaging often overlooks dysregulation in the absence of anatomical damage, a systems perspective reveals bile acids as dynamic regulatory signals linking the liver, gut, and microbiota. The diagram highlights the potential role of measuring fecal bile acids in providing a necessary window into this complex feedback loop, detecting the invisible regulatory instability that drives chronic symptoms despite normal standard tests.
Bile acids are usually discussed in narrow contexts for eg. Gallstones, Cholestasis or Fat malabsorption.
Outside these settings, they receive little clinical attention. When bowel symptoms appear without obvious structural disease, bile acids are rarely considered central to the problem.
But isn’t this a mistake?
From a systems perspective, bile acids are not merely digestive detergents. They are regulatory molecules that link the stomach, liver, intestine, microbiota, and nervous system into a functional axis. When this axis becomes unstable, symptoms emerge across regions that appear unrelated.
Understanding bile acid mediated disease requires stepping away from organ based thinking and towards functional integration.
Bile Acids as System Regulators
Bile acids are commonly described as fat emulsifiers but that description is incomplete.
They act as signaling molecules influencing intestinal motility, epithelial permeability, secretion, immune tone, and microbial composition. Through nuclear and membrane receptors, they regulate metabolism, inflammation, and transport. Their effects are dose dependent and context sensitive.
In a well regulated system, synthesis, transformation, reabsorption, and recycling occur in synchrony. The enterohepatic circulation maintains a dynamic equilibrium and when that equilibrium falters, symptoms follow.
The Enterohepatic System as a Regulatory Loop
Under normal conditions, bile acids circulate efficiently. They are synthesized in the liver, secreted into the intestine, modified by microbiota, reabsorbed primarily in the terminal ileum, and returned to the liver. Feedback mechanisms regulate synthesis based on reabsorption efficiency.
This loop depends on:
- Coordinated gastric and intestinal motility
- Intact ileal absorption
- Stable microbial transformation
- Functional feedback signaling
Disruption at any point alters downstream exposure and signaling intensity.
Regulation Failure Without Structural Disease
Bile acid mediated dysfunction does not require gross pathology. Functional failure alone is sufficient.
Disruption may arise from altered motility that changes delivery timing, from impaired ileal transport, from microbial imbalance that shifts bile acid composition, or from feedback failure leading to excess synthesis.
This results in an inappropriate bile acid exposure in the colon. Colonic bile acids stimulate secretion and motility and increase urgency, loosen stool consistency, and amplify postprandial responses. Patients experience diarrhea, bloating, abdominal discomfort, or unpredictable bowel patterns.
These symptoms are often labelled functional due to lack of any structural abnormality
The underlying mechanism however, is a regulatory failure.
Dysregulated Circulation, Not Just Malabsorption
The term bile acid malabsorption itself can be misleading.
In many patients, the issue is not absolute malabsorption but unstable circulation. Reabsorption may be incomplete or inconsistent, feedback signaling may fail to suppress synthesis or microbial conversion may favor more biologically active bile acid species.
Standard investigations often miss this entirely as endoscopies appear normal, there is nothing to be found in Imaging and neither the routine blood tests capture bile acid dynamics.
And ….the system fails quietly.
Bile Acids as One Signal Within a Network
Bile acids are not the only regulatory signals in the gut. They are used here as a clear and measurable example of how control signals shape system behavior.
Gastric acid secretion, pancreatic enzymes, incretin hormones such as GLP-1 and PYY, neuropeptides including substance P and VIP, serotonin-mediated enteric signaling, and vagal modulation all participate in similar regulatory loops. Each influences motility, secretion, permeability, and microbial interaction.
The principle is not that bile acids dominate the system, but that gut regulation is networked.
When one control signal destabilizes, others compensate, amplify, or adapt. Symptoms emerge from this interplay rather than from a single defect.
Why Symptoms Are Misclassified
Bile acid mediated bowel dysfunction often sits between specialties. It is not purely hepatic neither purely intestinal nor purely microbial. When frameworks are organ specific, network failures remain invisible.
Patients are told they have irritable bowel syndrome or functional diarrhea. Empirical treatments are tried and response becomes the diagnostic tool.
The absence of structural abnormality is often mistaken for absence of mechanism. In reality, many gastrointestinal disorders reflect regulatory instability long before tissue damage becomes visible
The Case for Measuring Fecal Bile Acids
One of the most striking gaps in gastrointestinal diagnostics is the lack of routine assessment of bile acid output.
Fecal bile acid measurement may provide a direct window into:
- Excess bile acid delivery to the colon
- Dysregulated enterohepatic circulation
- Functional malabsorption without structural disease
Unlike surrogate markers, fecal bile acids reflect the integrated result of synthesis, transformation, and reabsorption.
They do not specify where failure lies but they reveal that failure exists. Measuring fecal bile acids could help acknowledge a possible existence of Bile acid malabsorption or disorder of enterohepatic circulation.
In patients with chronic diarrhea, postprandial urgency, unexplained bloating, or refractory functional symptoms, this information can be decisive.
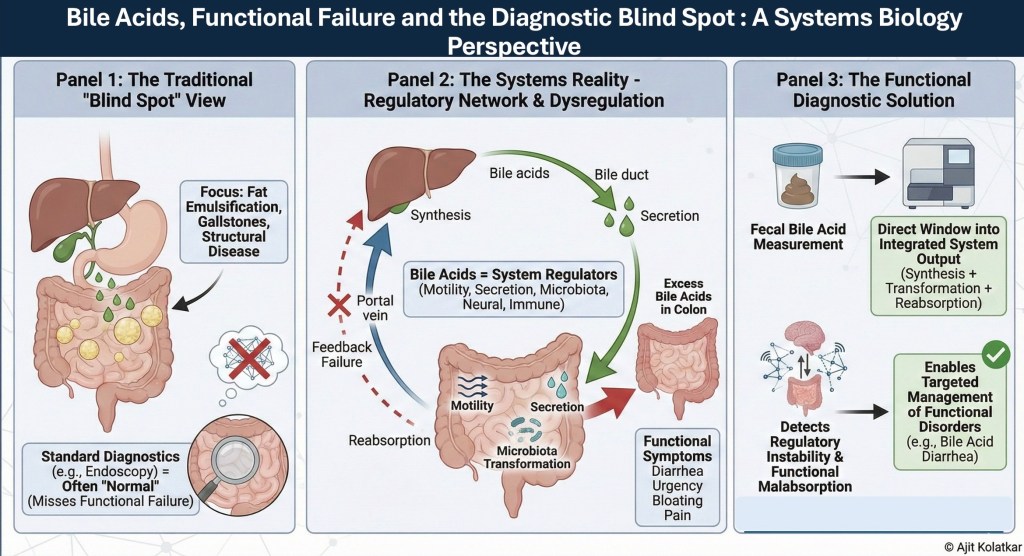
(Panel 1) Traditional diagnostics, such as endoscopy, prioritize structural pathology (e.g., gallstones or inflammation), creating a diagnostic “blind spot” for functional disorders where anatomy remains intact.
(Panel 2) A systems biology perspective reveals bile acids as critical regulatory signals influencing motility, secretion, and microbial balance. Disruption of the enterohepatic circulation—whether through feedback failure or transport instability—leads to functional symptoms like diarrhea and urgency without visible tissue damage.
(Panel 3) Fecal bile acid measurement may serves as a functional diagnostic tool. Unlike static imaging, it captures the integrated output of synthesis, transformation, and reabsorption, & may provide a window into regulatory failure.
A Systems Biology Perspective
From a systems biology standpoint, bile acids represent a control signal within a larger regulatory web.
They link liver output to intestinal behavior, microbial ecology, epithelial response, and neural signaling. They amplify disturbances when feedback fails.
Symptoms are not random but are patterned expressions of altered regulation.
Recognizing bile acid mediated dysfunction reframes bowel symptoms as part of a broader regulatory instability rather than as isolated functional disease. They lead to disorders that plausibly result from dysregulated enterohepatic circulatory
Looking Ahead
Bile acids are one entry point into understanding regulatory failure. They interact with motility, electrical rhythm, microbial networks, & metabolic feedback and demonstrate how symptoms migrate when coordination in the regulatory network is disturbed.
When regulatory signals are unstable, structure may remain intact but physiology and homeostasis get disrupted.
Functional disease requires functional measurement.
Bile acids should not be inferred……..but should be measured.

Leave a comment