Beyond Yes or No: Understanding GastroPanel as a Pattern-Based Test
When the heart suffers, symptoms are dramatic, and when the liver fails, blood tests change rapidly. The stomach, however, operates differently. It absorbs numerous insults over lifetime quietly, adapting and compensating for years. By the time symptoms become persistent, the underlying physiology may have already shifted significantly. That delay in visible signs is where most of the confusion around stomach disorders begins.
The Stomach Is Not Just an Acid Bag
We often reduce the stomach to a simple pouch responsible for acid production and indigestion. In reality, it is a highly regulated neuroendocrine organ. Stomach is lined by a sophisticated network of enteroendocrine cells that release neuropeptides that play a key role in human health and disease viz. serotonin, ghrelin, gastrin, obestanin, etc.
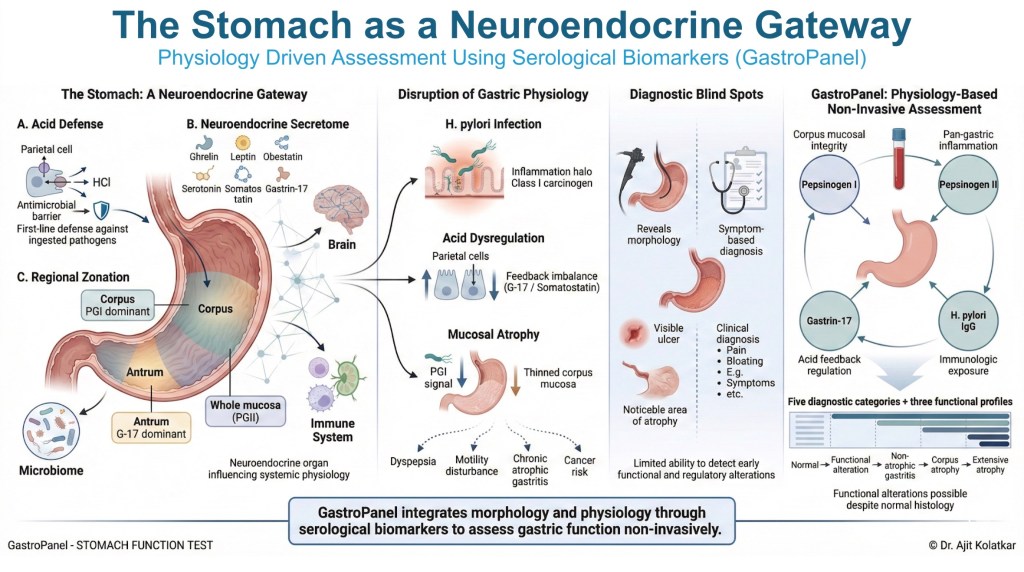
Parietal cells produce hydrochloric acid, chief cells secrete pepsinogens, G cells release Gastrin-17, and D cells produce somatostatin. These cells operate within a precise feedback loop that maintains the delicate balance between acid secretion, mucosal protection, and digestion.
Hydrochloric acid is not merely a corrosive substance; it protects against ingested pathogens and regulates the digestive process. Pepsinogens reflect the overall integrity of the gastric glands, while Gastrin-17 regulates acid output and reflects antral function.
When this complex system is disrupted, the stomach does not immediately collapse but it recalibrates. Acid levels may increase or decrease, hormonal feedback loops may shift, and inflammation can begin long before structural changes slowly evolve. Because symptoms during this phase may be mild, intermittent, or entirely absent, relying solely on how a patient feels is a highly unreliable diagnostic strategy.
The Silent Progression of Gastric Disease
Conditions such as Helicobacter pylori infection or atrophic gastritis often progress quietly. Clinical studies have shown that many individuals with atrophic changes remain asymptomatic for long periods. Standard endoscopy shows the physical structure of the stomach, but it does not show the underlying physiology. While a scope can easily detect visible erosions, ulcers, or severe atrophy, it cannot measure acid function, inflammatory dynamics, or hormonal feedback patterns.

This critical gap between functional physiology and visible structure is exactly where serological biomarker testing becomes relevant.
What GastroPanel Actually Measures

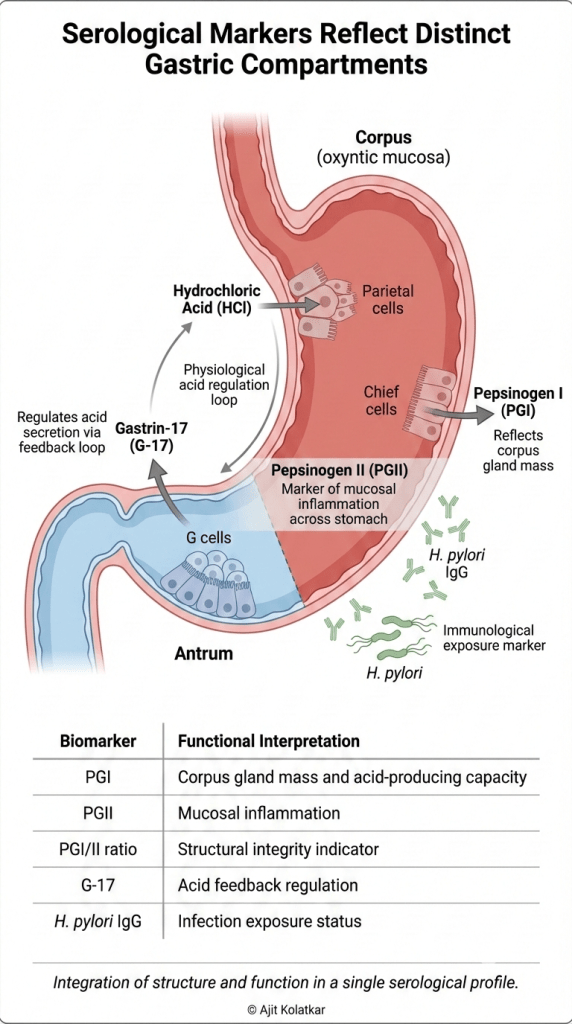
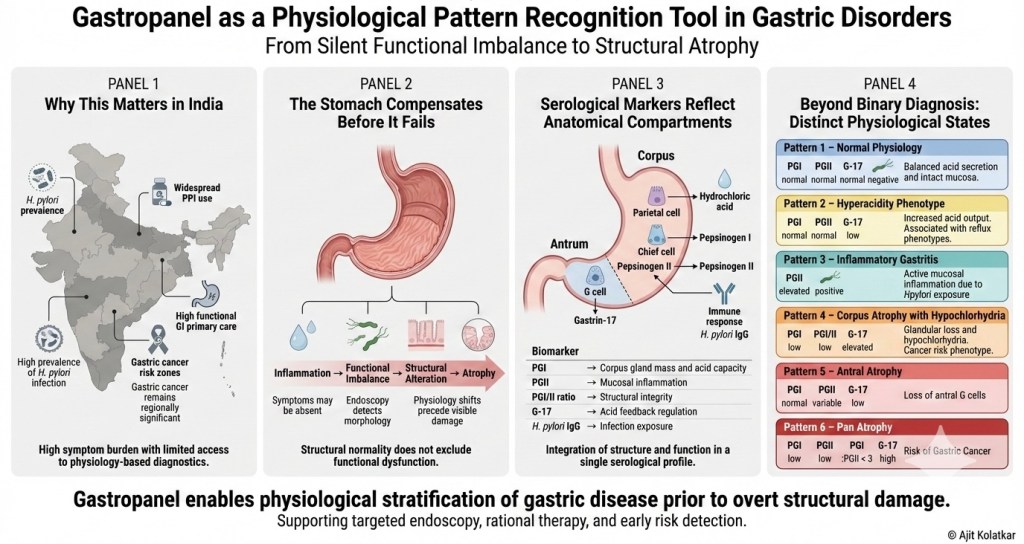
GastroPanel combines four key biomarkers that reflect both the function and structure of the gastric mucosa. Pepsinogen I serves as a marker of corpus gland mass and acid producing capacity. Pepsinogen II acts as a marker of mucosal inflammation across the entire stomach. The ratio between Pepsinogen I and II is a strong indicator of structural integrity, particularly for detecting corpus atrophy. Gastrin-17 reflects the acid feedback mechanism and overall antral mucosal function, while H. pylori IgG antibodies indicate current exposure or past infection status.
Each marker tells part of the story, and together they create a comprehensive physiological pattern.
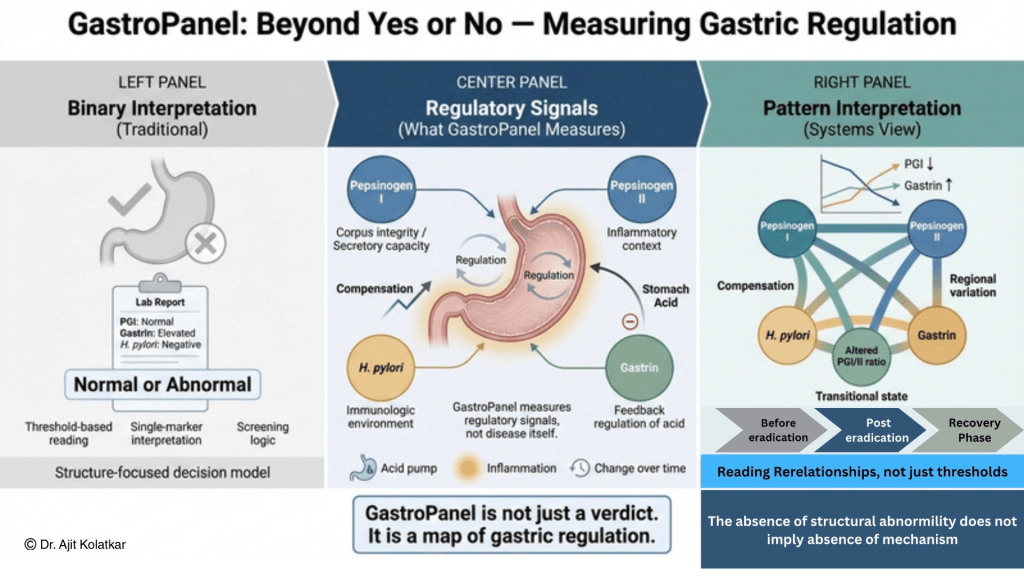
GastroPanel is not a binary test; it is a physiological map.
Moving Beyond Yes or No
Many patients approach diagnostics with a single question, wanting to know if they have something serious or not. GastroPanel does not simply offer a positive or negative verdict, but rather identifies specific physiological patterns.
A normal stomach physiology occurs when all markers fall within range, indicating no inflammation, no atrophy, and balanced acid function. This confirms physiological integrity rather than just the absence of disease.
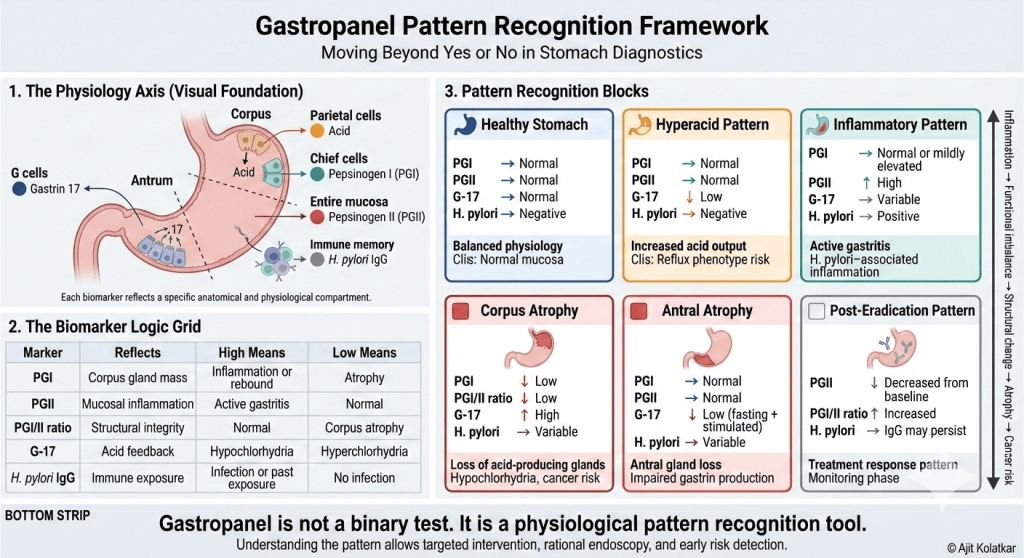
When we see a low Gastrin-17 level combined with normal pepsinogens, it often suggests increased acid output due to negative feedback suppression. This pattern is common in reflux phenotypes and certain presentations of gastroesophageal reflux disease. Conversely, an elevated Pepsinogen II suggests active mucosal inflammation, which is frequently associated with an active H. pylori infection. In the absence of an H pylori exposure or infection it may suggest that the inflammation is of non H pylori origin.
More advanced patterns further illustrate why Gastropanel cannot be interpreted as a simple positive or negative result.
A low Pepsinogen I together with a reduced PGI to PGII ratio strongly suggests corpus atrophy. In this state, the loss of parietal and chief cell mass leads to declining acid output. Hypochlorhydria develops gradually, and over time the long-term risk of gastric neoplasia increases.
When a low Pepsinogen I is accompanied by an elevated Gastrin-17, the interpretation becomes clearer. The rise in gastrin reflects compensatory feedback in response to reduced acid secretion. This pattern is consistent with hypochlorhydria secondary to significant corpus gland loss.
Conversely, a persistently low Gastrin-17 level in the context of long-term proton pump inhibitor exposure should not be dismissed. Under normal circumstances, sustained acid suppression leads to elevated gastrin due to feedback stimulation. If Gastrin-17 remains low despite prolonged PPI use, this raises concern for impaired antral G-cell function and suggests possible antral atrophy.
An even more severe phenotype emerges when both Pepsinogen I and Pepsinogen II are reduced, and the PGI to PGII ratio falls below 3. This constellation raises strong suspicion for pan-gastric atrophy involving both corpus and antral compartments.
It is this capacity for anatomical and functional localization that distinguishes Gastropanel from many other organ-based biochemical tests. Most laboratory panels, such as liver function tests, indicate the presence of injury but offer limited insight into regional physiology. Gastropanel, in contrast, provides compartment-specific information about the stomach, allowing clinicians to infer whether dysfunction is corpus-dominant, antral-dominant, inflammatory, or pan-gastric in nature.
This is not simply detection. It is localization.
Each of these patterns represents a distinct physiological state rather than a simple yes or no answer.
Why This Matters in Practice
In regions like India, dyspepsia is incredibly common, proton pump inhibitor use is widespread, and the prevalence of H. pylori remains significant. Consequently, many patients are treated empirically for months or even years without a clear understanding of their gastric function.
Gastropanel allows clinicians to identify
• Identification of hyperacidic states
• Recognition of hypochlorhydria
• Detection of inflammatory patterns
• Early identification of atrophic changes
• Better decision making about endoscopy
• Rational antibiotic use
It helps distinguish a healthy stomach from a diseased one, even when symptoms overlap
The absence of a structural abnormality should never be mistaken for the absence of a disease mechanism.
The Larger Perspective
The stomach rarely fails abruptly. It deteriorates through recognizable stages, beginning with inflammation, progressing to functional imbalance, then structural alteration, and eventually atrophy. By the time alarm symptoms appear, the disease process may already be advanced.
In India, this progression carries particular relevance. Gastric cancer continues to be diagnosed at late stages in a substantial proportion of patients, and five-year survival rates remain low. Dyspepsia is common, yet access to structured physiological evaluation remains limited. As a result, empirical therapy often substitutes for mechanistic understanding.
Within this context, Gastropanel represents more than another laboratory test. It introduces a physiology-based layer into the diagnostic pathway. It offers the possibility of identifying inflammatory states, acid dysfunction, and atrophic change before overt structural disease is visible.
There is a legitimate policy question here. Should a physiology-based serological panel be considered within broader gastric cancer prevention strategies in high-prevalence populations? That debate requires careful evaluation of cost-effectiveness, accessibility, and long-term outcomes. It is not a rhetorical question. It is a strategic one.
What is clear, however, is that GastroPanel shifts the clinical focus away from reactive symptom management toward structured physiological assessment. It moves the conversation from treating complaints to understanding compartments of dysfunction.
We are no longer merely labeling patients as dyspeptic. We are decoding the stomach, with the aim of intervening earlier and more intelligently.
Linking Back to the Larger Framework
Throughout this series, a consistent reasoning architecture has emerged.
Disease is widely recognised only when structure fails, even though functional compensation masks this instability much earlier.
Just as coordination can fail before movement stops, and bile acids can dysregulate without structural damage, gastric biomarkers can reveal altered regulatory states long before mucosal lesions appear. GastroPanel is a physiological language, and learning to read that language requires context, pattern recognition, and clinical humility.
Gastropanel represents one example of how a regulatory framework can be translated into practice. It is not the only tool. It is a demonstration of how pattern recognition can replace binary diagnosis in gastrointestinal medicine.

Leave a comment