In this essay, I use stomach disorders as a working model to illustrate a larger idea. The stomach is not unique in how it deteriorates. Many chronic diseases follow a similar trajectory of early regulatory disturbance, silent progression, and late structural manifestation. The gastroduodenal system, with its measurable biomarkers and clear feedback loops, allows us to see this progression distinctly. What we learn here extends far beyond the stomach.
The stomach rarely fails abruptly. It does not move from health to cancer in a dramatic leap. It changes gradually and often silently, adjusting its physiology long before structure reveals the consequences. The difficulty in modern gastroenterology is not that we lack technology. It is that we may be entering the story too late.
Are we recognizing gastric disease only after regulation has already begun to fail?
Most clinical frameworks remain oriented toward visible pathology. Ulcers, erosions, atrophy, intestinal metaplasia, and dysplasia are all structural landmarks. They are important, observable, and undeniable. Yet by the time they appear, the biological story has been unfolding for years.
If we are serious about early intervention, we must shift from detecting damage to staging dysfunction. This requires a different clinical approach. We must not simply ask what disease the patient has, but rather where along the continuum of physiological change the patient stands.
Disease Does Not Begin with Structure
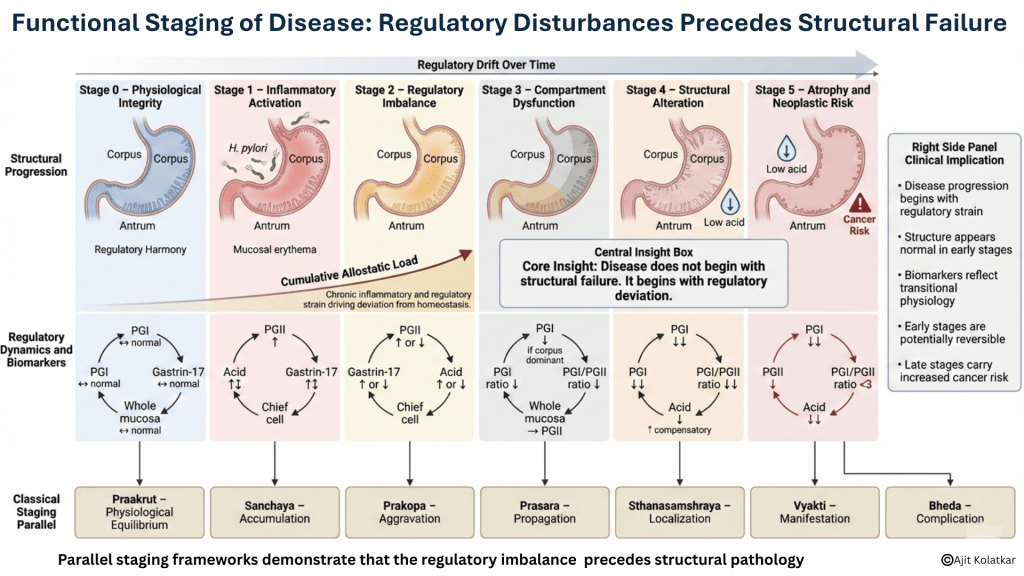
Gastric disease begins subtly. It often starts with inflammatory signaling, feedback shifts, and regulatory strain. The mucosa may still appear intact and endoscopy may be reassuring, while symptoms remain mild or inconsistent. Yet the system has already begun to recalibrate. Allostatic load is a frequently forgotten concept that constantly drives the body away from homeostasis.
Helicobacter pylori offers a clear example. Infection initiates inflammatory activity. Cytokine signaling alters acid secretion, gastrin dynamics shift, and pepsinogen patterns begin to change. The patient may experience vague dyspepsia or no symptoms at all. The process is active but not yet structurally destructive.
The stomach is a resilient organ. It tolerates repeated insults, compensates, and adapts acid production. It modifies feedback loops and redistributes secretory activity. These adaptive phases are precisely where staging becomes meaningful.
A Functional Staging Model of Gastric Disease
A practical way to conceptualize progression is to define stages that reflect physiology rather than morphology.
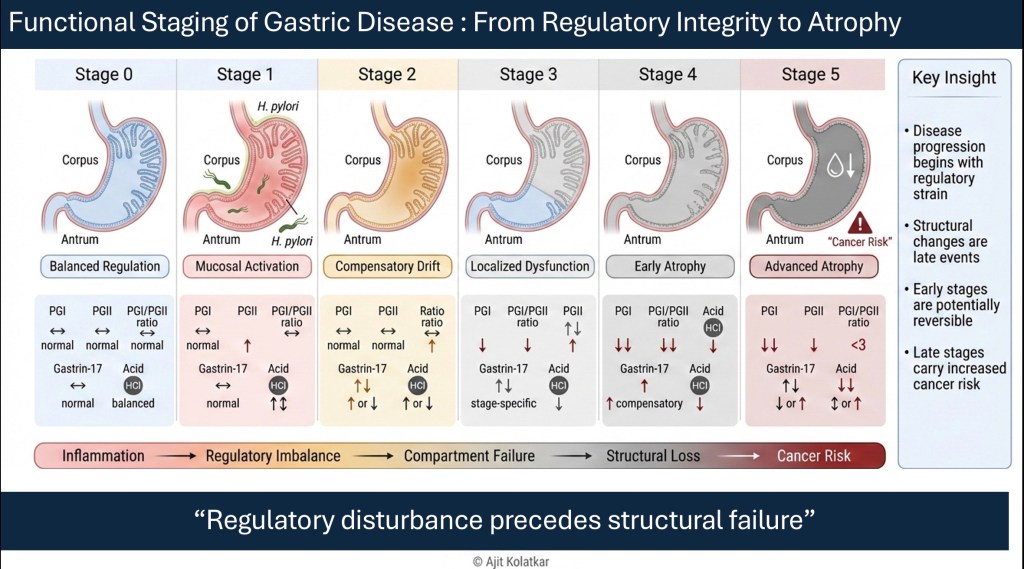
Stage 0 Physiological Integrity : Acid secretion is balanced, and gastrin feedback operates appropriately. Pepsinogen ratios reflect intact gland mass, and motility remains coordinated. Symptoms are absent or minimal. This is not merely the absence of disease; it is the presence of regulatory harmony.
Stage 1 Inflammatory Activation : Inflammation emerges, often driven by infection or environmental insult. Pepsinogen II may rise as a reflection of mucosal activation. Acid secretion may fluctuate, and feedback loops begin to strain. Symptoms may be intermittent, though structure remains largely preserved. This stage is frequently overlooked because visible damage has not yet appeared.
Stage 2 Regulatory Imbalance : Persistent inflammation or chronic exposure begins to alter regulatory set points. Gastrin levels adjust, and acid output may increase or decrease. Patients begin reporting functional symptoms such as fullness, reflux, early satiety, or bloating. The stomach is no longer operating at its original equilibrium. It is compensating. This is the phase where functional disorders are often labeled without an understanding of the underlying regulatory drift.
Stage 3 Compartment Dysfunction : The antrum and corpus may begin to behave differently. Acid producing capacity may decline in one region while inflammatory signaling persists in another. Feedback mechanisms become inconsistent. At this stage, patterns begin to localize. Corpus dominant dysfunction differs from antral dominant dysfunction. Acid feedback becomes distorted, and motility may become dyscoordinated. The structure may still appear grossly normal. This is where pattern recognition becomes clinically decisive.
Stage 4 Structural Alteration : Glandular mass begins to diminish. Pepsinogen I levels fall, and ratios shift. Hypochlorhydria develops more consistently, and atrophy becomes detectable histologically. The system can no longer compensate fully, and the regulatory architecture is visibly weakened.
Stage 5 Atrophy and Neoplastic Risk : Loss of gland mass becomes significant. Feedback loops collapse, hypochlorhydria persists, and the mucosal environment shifts. Long term cancer risk increases. Symptoms may or may not be dramatic, and the progression may still appear deceptively slow. By this stage, prevention becomes far more difficult.
Why Staging Matters
Without staging, patients are grouped simplistically. They are labeled as dyspeptic, reflux prone, functional, or gastritic. These labels describe symptoms rather than trajectory.
Staging provides context and answers the question of direction. It tells us if the stomach is moving toward recovery or deterioration. It clarifies whether inflammation is transient or entrenched, and if regulatory imbalance is reversible or structurally fixed. It also reframes screening.
If we recognize that disease evolves through predictable regulatory transitions, we can intervene before structural decline becomes irreversible.
Shatkriyakaal and Functional Staging: A Structured Parallel
Long before modern physiology described allostasis, regulatory drift, and cumulative strain, classical Ayurvedic texts described disease progression through a staged framework known as Shatkriyakaal. This model does not begin with pathology. It begins with equilibrium.
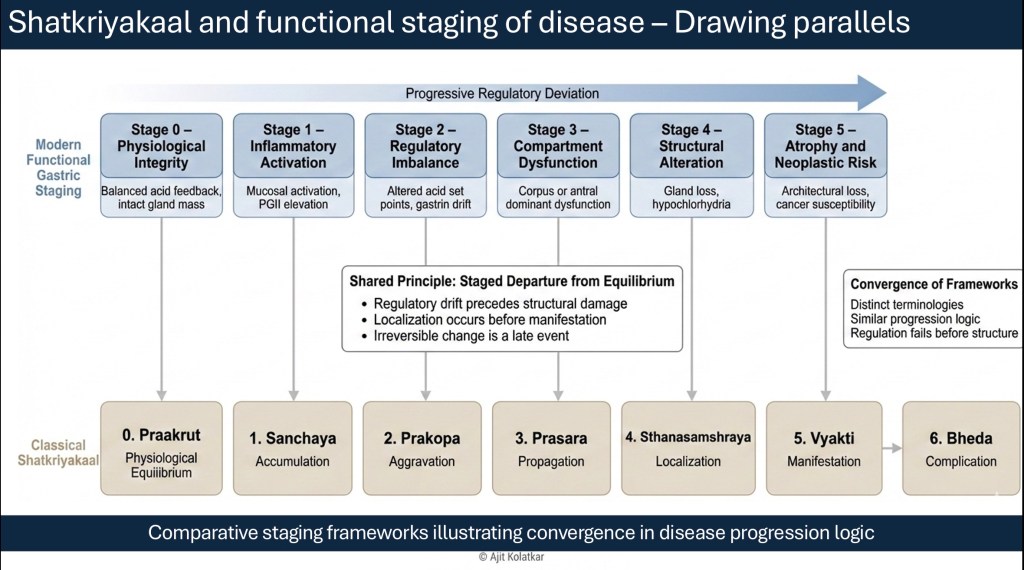
The baseline state is described as Praakrut, a condition of physiological harmony in which regulatory mechanisms function appropriately and tissues maintain structural integrity. Disease does not begin abruptly from this state, but rather begins with deviation.
The first stage, Sanchaya, represents accumulation. In gastric terms, this corresponds to early inflammatory activation or subtle biochemical shifts that precede structural injury.
The second stage, Prakopa, reflects aggravation. Regulatory imbalance intensifies, acid feedback loops begin to drift, and hormonal signaling becomes strained.
The third stage, Prasara, denotes propagation. Dysregulation extends beyond its original locus. In the stomach, this appears as emerging compartmental dysfunction where the corpus and antrum begin to behave differently.
The fourth stage, Sthanasamshraya, signifies localization. Regulatory failure anchors within the tissue, and structural alteration begins to appear as glandular mass declines.
The fifth stage, Vyakti, represents manifestation, where disease becomes clinically and structurally apparent.
The sixth stage, Bheda, indicates complication. At this point, irreversible change and long term risk become evident.
The language differs from contemporary gastroenterology, but the staging logic converges. Both frameworks recognize that disease evolves through progressive regulatory imbalance before structural collapse.
So it is not a philosophical equivalence; it is a structural parallel.
The Cost of Ignoring Early Stages
When we focus only on structure, we enter the disease process at Stage 4 or Stage 5. At that point, prevention is reactive rather than proactive.
In high prevalence regions where dyspepsia is common and gastric cancer is often diagnosed late, the absence of structured physiological staging represents a major diagnostic gap. Empirical therapy may temporarily relieve symptoms, but without understanding the stage, we may miss progression. Staging introduces accountability into clinical reasoning. It demands that we ask not only what is visible, but what is evolving.
Functional Staging Is a Clinical Tool
Functional staging does not replace endoscopy or histology. It contextualizes them. It integrates biomarker interpretation, symptom patterns, infection status, and regulatory feedback into a longitudinal view. It changes the conversation from asking whether a patient has a disease to asking where a patient is in the disease process. That shift is subtle, but transformative.
Looking Forward
If gastric disease unfolds through regulatory stages rather than isolated events, then viewing the stomach as a single organ acting independently becomes insufficient. The regulatory signals that define each stage interact with motility, bile acid circulation, the microbiota, and neural coordination.
The next step is to move beyond compartmental thinking and examine how organ based medicine gives way to network based understanding. When regulation fails, it rarely fails in isolation. Understanding that shift requires us to rethink the organ itself.
Functional staging is not the end of the reasoning process; it is the beginning of systems thinking.

Leave a comment