There is a quiet discomfort that many clinicians experience but rarely articulate. It emerges in those moments when a patient sits across the table describing persistent symptoms while every investigation appears normal. Every scan looks reassuring, every report suggests that nothing is wrong. Yet, something clearly is.
This discomfort is not a failure of medicine, but rather a limitation of the school of thought using which we are trained to see the human body. Modern medicine has been built with extraordinary precision around the idea that disease belongs to isolated organs. We are taught that each organ has a defined structure and function, and that pathology can be located, visualized, and treated within that strict anatomical boundary.
This approach has given us remarkable success in conditions where structure is visibly altered; such as tumors, ulcers, strictures, or fibrosis. In these cases, the problem can be seen, measured, and directly addressed. But this lens begins to lose clarity in a different category of illness. It falters when symptoms are real, distressing, and persistent, yet structure remains deceptively normal.
The Limits of Seeing Through Structure
When a patient presents with bloating, reflux, fatigue, or overlapping symptoms that shift across systems, our instinct is to look for structural explanations. We search for inflammation, erosion, obstruction, or biochemical abnormalities to anchor the diagnosis. But very often, these findings are either entirely absent or vastly insufficient to explain the full clinical picture.
This is the space where functional disorders reside. It is also the space where the traditional organ-based model begins to reveal its boundaries. The model assumes that function is a direct consequence of structure. Biology, however, often behaves in a far more dynamic and interconnected way.
What becomes evident over time is that structure alone cannot explain function. Function is not confined to a single organ. It emerges from continuous interactions across multiple systems that communicate, adapt, and regulate each other in ways that are not always visible on conventional tests.
The Body Is Not a Collection of Organs
What we refer to as organs are, in reality, nodes within a much larger network. Anatomy allows us to separate them for the purpose of study, but physiology constantly reconnects them through shared signals, feedback loops, and regulatory pathways.
The stomach does not function in isolation when it secretes acid. That secretion is influenced by neural inputs, hormonal signals such as gastrin, and feedback from the duodenum. All of these are shaped by what is being ingested and how the rest of the system is responding.
The liver does not simply process fat in isolation. It receives a continuous stream of metabolites from the gut through the portal circulation. Those metabolites are themselves products of microbial activity, dietary inputs, and intestinal barrier function.
Even the intestine is not just a site of absorption. It hosts a complex ecosystem of microorganisms that generate a wide array of bioactive compounds. These compounds influence immune responses, neural signaling, and metabolic pathways far beyond the confines of the gut. What appears anatomically separate is physiologically continuous. Once this continuity is appreciated, the idea that disease can be fully understood within a single organ begins to feel increasingly incomplete.
Regulation Is Distributed, Not Localized
One of the most important shifts in thinking comes from recognizing that biological regulation is not centralized in one location. It is distributed across systems. Signals originate in one place, are modified in another, and often manifest in a third location that may seem unrelated at first glance.
This distributed regulation explains why a disturbance in the gut can influence the liver. It explains why immune activation at a mucosal surface can precede autoimmune disease elsewhere in the body. And it explains why symptoms overlap across gastrointestinal, neurological, and metabolic domains without a single unifying structural abnormality.
This is why a failure in the gut’s electrical rhythm can stall digestion without any visible blockage. It is why a misfiring bile acid feedback loop can cause severe, unpredictable diarrhea despite a perfectly normal endoscopy.
It also explains a phenomenon that patients frequently describe but find difficult to articulate: their symptoms do not stay confined to one region. Instead, they seem to migrate, evolve, and overlap over time in ways that feel unpredictable.
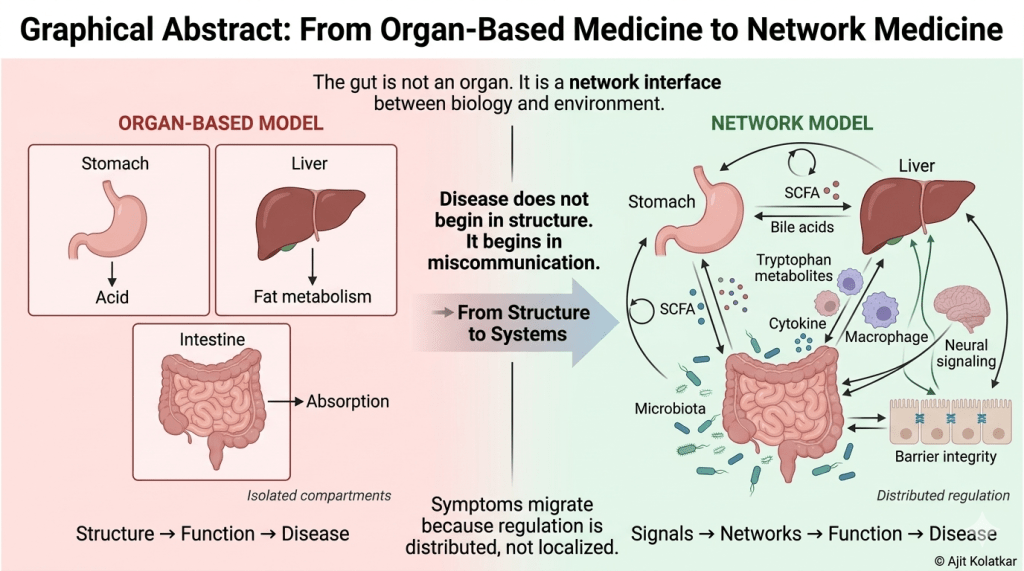
Symptoms migrate because regulation is distributed, not localized.
The Role of Feedback and Compensation
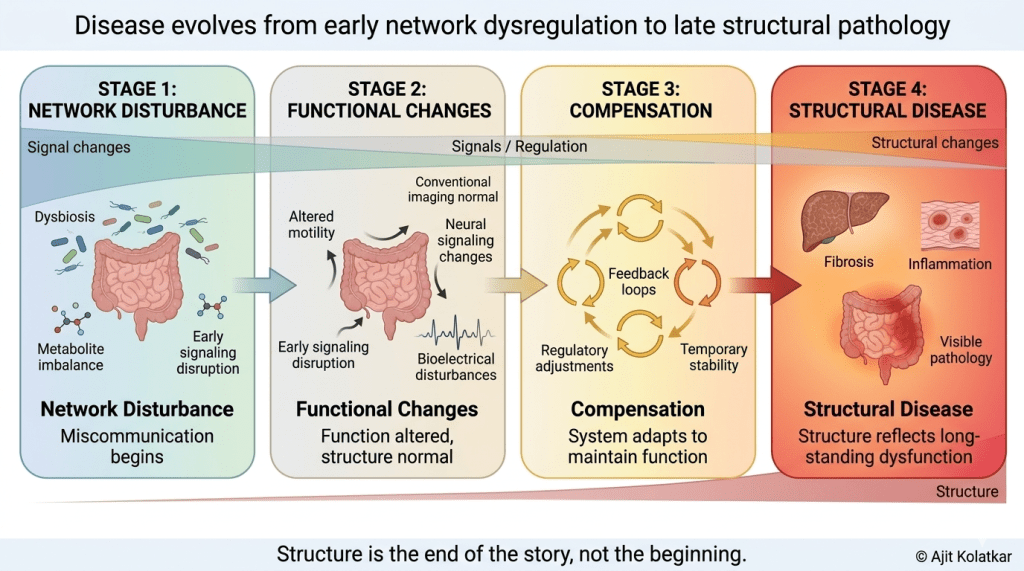
Living systems are not static. They are constantly adjusting to internal and external changes through feedback mechanisms that allow them to maintain balance. This is why early dysfunction is often compensated for rather than immediately expressed as overt disease.
When one pathway becomes inefficient, another adjusts to maintain function. This compensation can persist for long periods of time, creating a state where the system is functioning, but not optimally. Subtle symptoms begin to emerge long before any structural damage becomes apparent.
This is why many chronic conditions appear to develop slowly. By the time structural changes are finally detected on a scan, the underlying dysregulation has often been present for years, quietly shaping the trajectory of the disease.
The Gut as a Central Interface
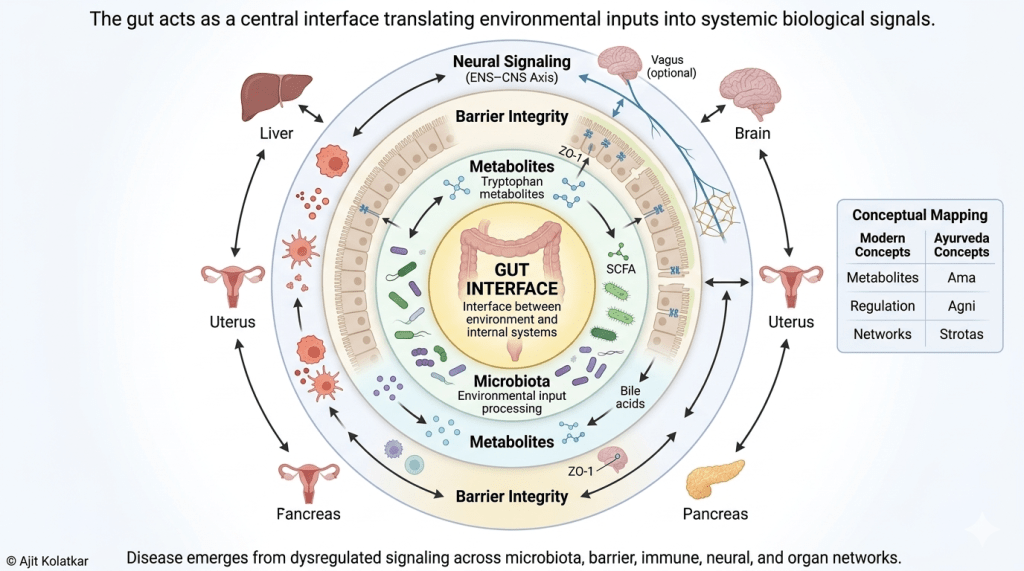
At the center of this networked view of biology lies the gastrointestinal tract. It is uniquely positioned at the interface between the external environment and the internal systems of the body.
Every day, the gut is exposed to dietary inputs, microbial communities, and environmental factors. Simultaneously, it communicates with the immune system, the nervous system, and metabolic pathways. This makes it one of the most dynamic and responsive systems in the body.
The metabolites produced by gut microorganisms including short-chain fatty acids, bile acid derivatives, and tryptophan metabolites are not passive byproducts. They are active signals that influence inflammation, energy metabolism, and even brain function.
The integrity of the intestinal barrier determines how these signals are regulated. When the barrier functions well, it allows selective communication. When it becomes compromised, it permits the translocation of microbial products that can trigger massive immune activation and systemic effects.
The gut is not an organ. It is a network interface between biology and environment.
Disease as Miscommunication
When viewed through this paradigm, disease begins to look less like a localized structural defect and more like a breakdown in communication across networks. Signals are either distorted, amplified, or inadequately regulated.
This miscommunication can occur at multiple levels—including microbial composition, metabolite production, barrier function, immune signaling, and neural regulation. It is the cumulative effect of these disturbances that eventually manifests as symptoms and, much later, as structural disease.
By the time we detect visible changes in an organ, the underlying communication network has often been disrupted for a significant period. This is why focusing only on structure may address the consequence but not the root cause.
Disease does not begin in structure. It begins in miscommunication.
From Organs to Networks
This realization does not invalidate organ-based medicine, but it extends it. It asks us to move beyond isolated compartments and begin to see the body as an interconnected system where function emerges from relationships rather than from individual parts.
Interestingly, this shift toward network thinking is not entirely new.
In many ways, this movement toward network medicine finds a natural resonance within Ayurveda. In this ancient system, the body has never been viewed as a collection of isolated organs. Instead, it is an interconnected system governed by dynamic principles of regulation and balance.
Concepts such as Agni which represents the body’s capacity to transform and regulate inputs, and Ama, which reflects the accumulation of improperly processed or dysregulated signals; offer a framework that aligns closely with modern ideas of metabolic control, immune activation, and systemic dysfunction.
The idea of Srotas, or channels of flow and communication, further reinforces the notion that physiology operates through networks rather than compartments. Disturbances in one pathway seamlessly influence distant systems through interconnected signaling. Rather than locating disease within a single organ, Ayurveda emphasizes patterns of imbalance across systems, recognizing that dysfunction often begins at the level of regulation and only later manifests as structural change.
In this sense, what we are now describing as network physiology and systems medicine can be seen as a contemporary language for principles that have long acknowledged the body as an integrated, adaptive, and continuously communicating whole.
It invites us to ask different questions: not only about where a disease is located, but about how systems are interacting, which signals are altered, and how regulation has shifted over time. It also opens the door to new approaches in diagnostics and treatment that focus on restoring balance within networks rather than simply correcting structural abnormalities.
A Necessary Shift in Perspective
The transition from organ-based medicine to network medicine is not a rejection of what we know. It is an evolution of how we understand it. It acknowledges that structure provides only part of the story, while function, regulation, and communication provide the rest.
To truly understand disease, we must learn to see beyond what is visible. We must recognize patterns across systems and appreciate that the body is not a collection of isolated organs, but a continuously interacting network that responds to both internal and external influences.
And perhaps most importantly, it reminds us of a vital clinical truth: when patients describe symptoms that do not fit neatly into structural categories, they are not presenting a mystery to be dismissed. They are presenting a signal to be understood within a broader and more connected framework.

Leave a comment