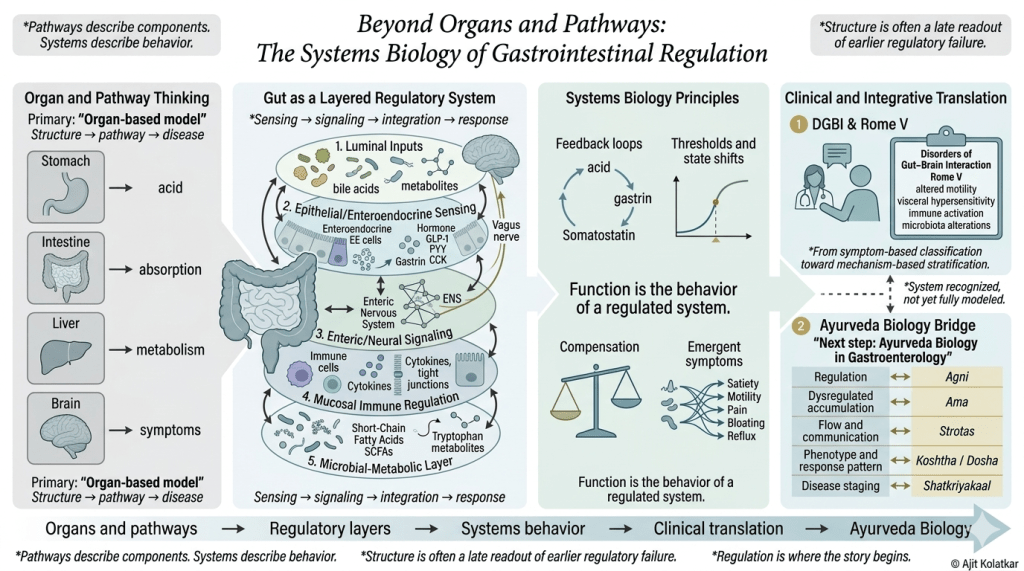
For decades, gastroenterology has relied on an organ-based, linear model of disease: structure dictates pathway, and pathway dictates symptom. But the gut does not function in isolated boxes. It is a highly adaptive, layered regulatory system where luminal inputs, immune responses, the microbiome, and the enteric nervous system constantly communicate.
Pathways describe components, but systems describe behavior.
This graphical abstract maps the critical shift from looking at isolated structural damage to understanding regulatory dynamics. By applying systems biology principles—like feedback loops, thresholds, and compensatory masking—we can better understand Disorders of Gut-Brain Interaction (DGBI) and move from symptom-based classification toward mechanism-based stratification.
There is a familiar clinical moment that many of us recognize where a patient describes persistent symptoms that are real, often disabling, and clearly evolving over time, clinical examinations reveal nothing much of significance, the structure appears intact, and the explanation that we get leaves us unsatisfied. But the question that comes to my mind is that are we looking at the right level of biology.The gastrointestinal system invites that question more than most. It is accessible, measurable, and deeply studied, yet it continues to produce patterns of disease that do not fit neatly within structural boundaries.
To understand why, we have to move beyond the idea that function is simply what an organ does, and begin to see it as what a system achieves through regulation.
From Pathways to Systems
Much of what we learn about physiology is organized as pathways. A hormone is released, a receptor is activated, a response follows. This way of thinking is precise and necessary, but it could be incomplete. What pathways best describe could be thought of as components but systems on the other end describe behavior.
Systems biology asks a different set of questions;
How do multiple pathways interact over time?
How does a system maintain stability in the face of constant change?
What happens when feedback becomes strained, delayed, or excessive?
Why does a small disturbance sometimes produce a large effect, while a larger disturbance is absorbed without visible consequence?
The language that emerges from this way of thinking includes feedback loops, thresholds, nonlinear transitions, compensation, and emergent properties which are not abstract ideas. They are the grammar of how living systems actually function.
The Gut as a Layered Regulatory System
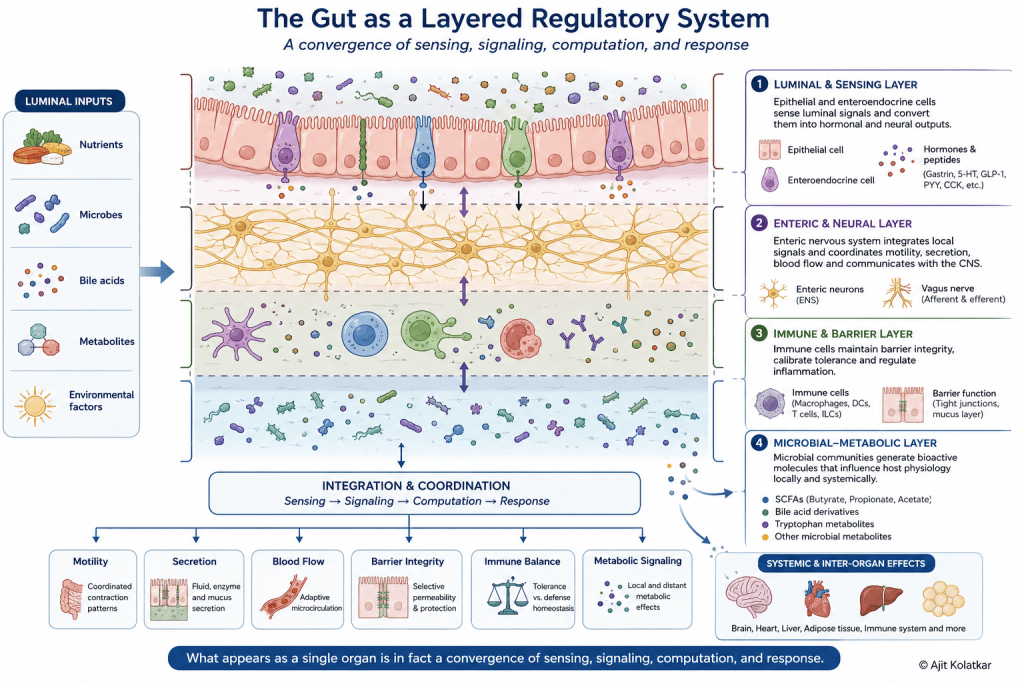
The gastrointestinal tract is often described as a tube with specialized segments, each performing a defined task. In reality, it behaves more like a layered regulatory system in which multiple processes operate simultaneously and continuously influence each other.
At the luminal level, the gut is exposed to nutrients, microbes, and environmental inputs that are not passively processed. They are sensed where specialized epithelial and enteroendocrine cells detect chemical signals and translate them into hormonal and neural outputs.
Beneath this layer lies a dense network of neurons forming the enteric nervous system, which integrates local signals and coordinates motility, secretion, and blood flow. Alongside it operates the immune system, which does not simply defend against pathogens but continuously calibrates tolerance and response based on what the mucosa encounters.
Overlaying all of this is the metabolic layer, where microbial communities generate a wide range of bioactive molecules that influence host physiology. These molecules do not remain confined to the gut. They circulate, interact with distant organs, and shape systemic behavior.
What appears as a single organ is in fact a convergence of sensing, signaling, computation, and response.
Sensing Before Responding
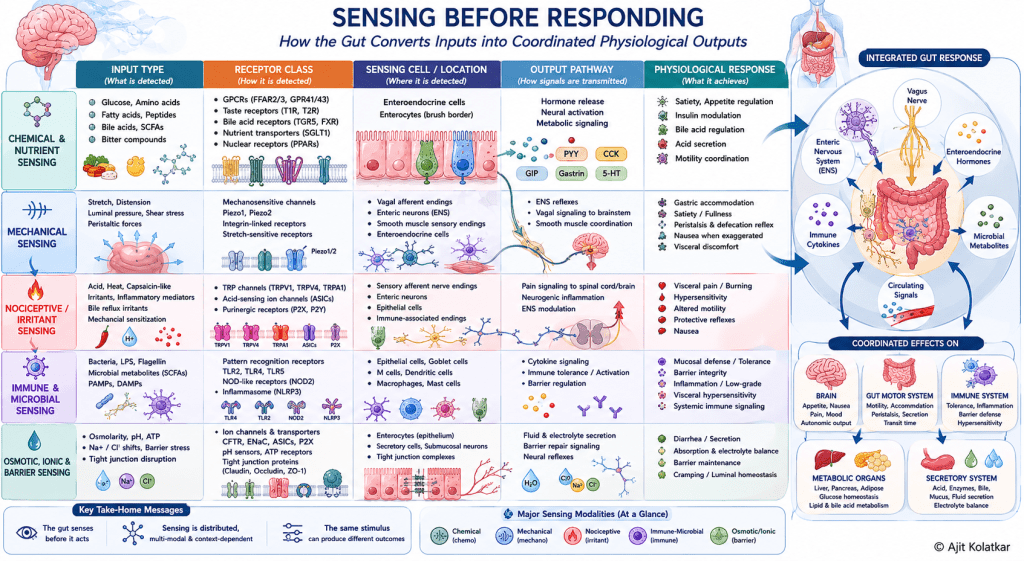
It is of importance to note that the gut senses before it acts. Enteroendocrine cells, often described as hormone-secreting cells, better understood as transducers detect luminal signals and convert them into coordinated outputs that influence digestion, appetite, motility, and inter-organ communication.
This sensing is distributed, varies by region and is influenced by prior exposure, microbial composition, and systemic state. The same stimulus can produce different responses depending on the context in which it is encountered.
The gastrointestinal system is state dependent meaning that the GI responses are shaped not only by the stimulus itself but by the condition of the system receiving the stimulus. The same food, metabolite, stretch or microbial signal may produce different outputs depending on inflammation, motility, microbiome, neural tone, barrier integrity and prior exposure. And there the GI system should not be reduced to mere fixed pathways.
Feedback as the Core of Regulation
At the heart of gastrointestinal physiology lies feedback. Acid secretion is not simply produced but is regulated through loops involving gastrin, somatostatin, neural inputs, and luminal signals. Likewise motility is not a simple contraction but is coordinated through interactions between smooth muscle, pacemaker cells, neural circuits, and downstream resistance.
Though these loops stabilize function they do tend to create vulnerability.
Meaning when feedback is precise, the system remains balanced but when it becomes delayed, exaggerated, or uncoupled, it becomes dysregulated. This drift may not be immediately visible in structure but can be experienced as altered function.
Thresholds and Nonlinear Behavior
One of the reasons gastrointestinal disorders are difficult to interpret is that they do not always behave proportionally. Small changes can produce large symptoms, while significant disturbances may remain clinically silent for a time. And this exactly is the hallmark of nonlinear systems. There are thresholds beyond which behavior changes abruptly, states that appear stable until they are not while transitions that are not gradual but sudden.
A patient may function within a compensated state for years, only to experience a rapid shift in symptoms once a threshold is crossed. What appears as a new disease may in fact be a change in system state.
Compensation and the Masking of Failure
Living systems are designed to adapt. When one pathway becomes inefficient, others adjust to preserve overall function. This compensation is essential for survival and is also one of the reasons why early disease is difficult to detect. The gastrointestinal system can maintain outward function despite internal dysregulation. Acid levels may be preserved through hormonal adjustment. Motility may adapt to maintain transit. Immune responses may recalibrate to contain disturbance.
This creates a phase where the system is working, but not working well. Symptoms emerge in this phase, often without clear structural explanation. By the time structural changes appear, the system has already been under strain for a prolonged period.
Emergent Properties of Gastrointestinal Function
When multiple layers interact, new behaviors emerge that cannot be predicted by studying each component in isolation. Satiety, for example, is not the result of a single hormone but is the integrated outcome of luminal sensing, enteroendocrine signaling, neural feedback, and central processing. Similarly, coordinated propulsion depends on the interaction of electrical rhythms, muscle activity, neural control, and downstream resistance. Disruption in any one of these can alter the whole pattern. All these are emergent properties and belong to the system, not to any single part.
Function is not the output of an organ but behavior of a regulated system.
Control Signals and System Behavior
Across these layers, certain signals act as regulators. Hormones, neurotransmitters, microbial metabolites, and cytokines all serve as control inputs that shape system behavior. Their effect is not fixed but dependent on timing, concentration, receptor sensitivity, and the state of the system.
Disease can arise when these signals are excessive, insufficient, mistimed, or misinterpreted. It can also arise when the system becomes less responsive to them. And this is not a failure of a single pathway but is dysregulation.
Structure, in this context, becomes a late readout. It reflects what has already been unfolding at the level of signaling and feedback.
Why This Matters Clinically
When we view the gastrointestinal system through this lens, several observations begin to make sense.
Why do patients have symptoms despite normal investigations?
Why do different disorders share overlapping features?
Why are treatment responses variable?
Why is early intervention difficult using structure-based diagnostics alone?
It also changes the questions we ask. Instead of asking which organ is diseased, we begin to ask which regulatory layer is disturbed, which physiological pathways are altered, and how the system has adapted over time.
Once gastrointestinal symptoms are understood as expressions of altered regulation rather than isolated organ failure, it becomes clear why clinical frameworks themselves are beginning to change. This is where the evolution of Disorders of Gut–Brain Interaction and the Rome V framework becomes important.
It is beginning to reshape how gastroenterology classifies functional disorders, especially through the evolving framework of Disorders of Gut–Brain Interaction and Rome V.
Systems Thinking in Clinical Frameworks: The Evolution of DGBI and the Rome V Perspective
The shift toward systems thinking is not limited to theoretical biology. It is beginning to appear within clinical gastroenterology as well.
The evolution of disorders now described as Disorders of Gut–Brain Interaction reflects this transition. These conditions were earlier grouped under functional gastrointestinal disorders, a term that often implied the absence of structural disease without fully explaining the underlying biology. The newer framing recognizes that these are not merely diagnoses of exclusion, but disorders rooted in altered regulation across interacting systems.
The Rome V framework is an important step in this direction. It acknowledges that gastrointestinal symptoms may arise from altered motility, visceral hypersensitivity, immune activation, mucosal barrier changes, microbiota alterations, and central nervous system modulation. This is a clear movement away from single-organ explanations toward a more integrated view of gastrointestinal physiology.
In many ways, this aligns with systems biology. Bidirectional gut–brain signaling, microbial metabolites, immune–neural interaction, and barrier function all point toward a distributed regulatory model rather than a localized structural defect.
However, there remain important gaps.
Much of the framework still relies heavily on symptom-based classification. This is clinically practical, but it does not fully capture the underlying regulatory state of the patient. Objective physiological markers, biomarker patterns, motility signatures, mucosal immune signals, and microbial-metabolic profiles are still not integrated into routine classification in a meaningful way.
The framework recognizes the system, but the system is not yet fully modeled.
This creates an opportunity to move beyond descriptive classification toward mechanism-based stratification, where patients are understood not only by symptoms, but by their position within a dynamic regulatory landscape. What remains is the integration of these concepts into everyday clinical reasoning.
A Direction Forward
The move towards systems biology does not discard what we know but it builds on it. It allows us to integrate molecular detail with physiological behavior and clinical observation.
It also creates a bridge towards frameworks that have long emphasized regulation over structure, pattern over location, and process over static definition. This is where Ayurveda Biology becomes especially relevant, not as a return to the past, but as a way to reinterpret classical physiological concepts through the language of systems science.
Concepts such as Agni, Ama, Strotas, Dosha, Koshtha, and Shatkriyakaal can be revisited not as isolated traditional terms, but as process-based frameworks that speak through regulation, accumulation, flow, phenotype, and staged disease progression.
The next step in this series is therefore to examine how Ayurveda Biology can contribute to gastroenterology, not by replacing modern science, but by expanding the way we understand regulation, resilience, and disease evolution.
For now, it is enough to recognize that the gastrointestinal system is not a collection of parts performing isolated functions but a dynamic, adaptive system that senses, integrates, and responds across multiple layers.
Structure is often what we see at the end, regulation is where the story begins.

Leave a comment