In the previous blog, I examine the gastrointestinal system as a dynamic regulatory network rather than a collection of isolated organs and pathways. The next question that comes to my mind is whether there could be frameworks that could understand physiology through regulation, transformation, flow, phenotype, and staged progression?
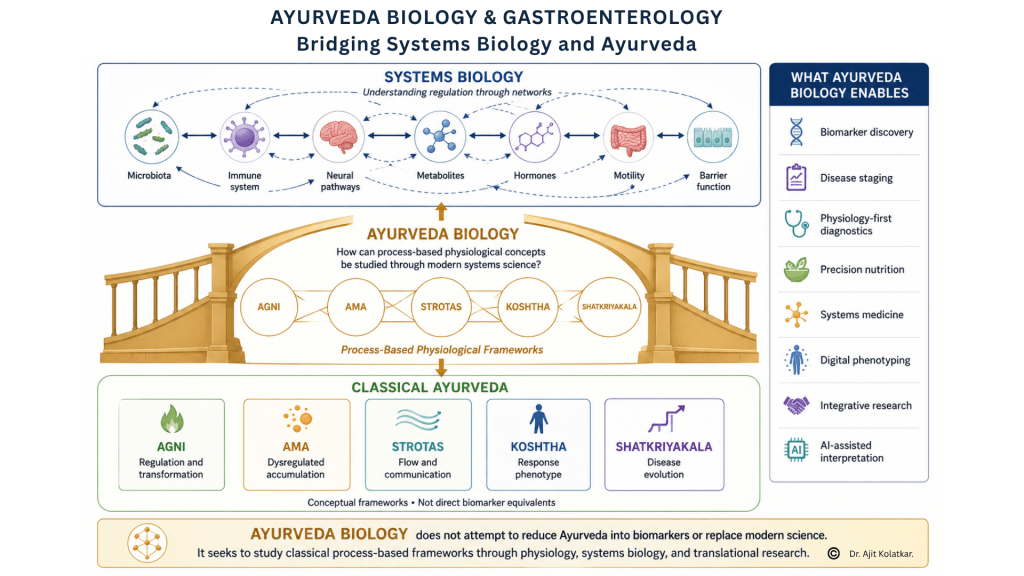
Ayurveda Biology enters at this juncture, not as a rejection of modern gastroenterology, but as a way to reinterpret classical Ayurvedic physiological concepts through the language of systems science and this is an important distinction. Ayurveda Biology is not an attempt to force ancient terminology into modern biomedical categories, nor is it an effort to reduce complex Ayurvedic ideas into single biomarkers or isolated mechanisms. It is a transdisciplinary approach that asks whether classical concepts can be studied, interpreted, and applied through physiology, systems biology, clinical reasoning, and modern research tools.
If systems biology gives us the scientific grammar of regulation, Ayurveda offers an older clinical language of regulation, adaptation, imbalance, and staged disease.
Ayurveda Biology Is Not a Return to the Past
There is a tendency to place Ayurveda and modern medicine in opposition, as if one must choose between traditional wisdom and contemporary science. I find that approach too narrow. The more meaningful opportunity lies in asking how different knowledge systems can illuminate different levels of biological organization.
Modern gastroenterology has become extraordinarily powerful at identifying structural disease, molecular targets, inflammatory pathways, infections, malignancy, and organ-specific dysfunction. It has transformed the diagnosis and treatment of many conditions. Yet, as discussed earlier in this series, it still struggles in areas where symptoms arise from altered regulation rather than visible damage.
Ayurveda, on the other hand, has historically approached health and disease through patterns of function, digestion, transformation, flow, resilience, constitution, and progression. Its terminologies or language is different, but its clinical attention is often directed towards process rather than isolated structures.
One of its purpose is to examine whether concepts such as (but not limited to) Agni, Ama, Strotas, Dosha, Koshtha,Shatkriyakala, etc. can be studied in relation to measurable physiology, biomarkers, microbiome patterns, metabolic states, motility profiles, immune regulation, and disease trajectories.
Agni as Regulatory Competence
Agni is often translated simply as digestive fire, but that translation is too limited for a systems biology interpretation. In a broader physiological sense, Agni can be understood as the body’s capacity to transform inputs into usable biological outputs while maintaining internal order.
Classical Ayurvedic texts describe Agni not merely as a digestive force, but as a principle responsible for Vivechana (discrimination), Pachana (transformation), and Munchana (appropriate release and elimination). In other words, Agni determines what should be accepted, what should be transformed, what should be assimilated, and what should be discarded. From a contemporary point of view, these functions extend far beyond digestion and resemble the fundamental regulatory tasks performed by biological systems.
In gastroenterology, this begins with digestion, but it does not end there. Food must first be sensed and evaluated. Acid and enzymes must be secreted at the appropriate time and in the appropriate amount. Bile and pancreatic responses must be coordinated. Motility must regulate the movement of luminal contents. Nutrients must be selectively absorbed. Microbial metabolites must be interpreted and integrated. Potentially harmful signals must be contained, while useful signals are incorporated into systemic physiology.
Seen this way, Agni is not one function. It is a regulatory capacity that spans discrimination, transformation, assimilation, metabolism, neuroendocrine signaling, microbial interaction, immune regulation, and systemic adaptation.
This interpretation allows us to ask more precise questions. Is digestive capacity impaired? Is acid output excessive or insufficient? Is bile flow appropriate? Is pancreatic response adequate? Is motility coordinated? Is microbial metabolism supporting or disturbing host physiology? Is the system able to distinguish beneficial from harmful signals and adapt appropriately to dietary, environmental, and metabolic demands?
Ama as Dysregulated Accumulation
Ama is another concept that is often oversimplified. It is sometimes described as a toxin, but that translation can be misleading because it suggests a single substance that can be directly measured. A more useful interpretation is to view Ama as a pattern of dysregulated accumulation arising from impaired processing, incomplete transformation, altered clearance, or disturbed biological communication.
From a systems biology perspective, Ama may be better understood as an emergent phenomenon rather than a discrete entity. Instead of representing a single molecule, Ama may be also thought of a dynamic dysregulated interactome and secretome composed of microbial products, metabolic intermediates, inflammatory mediators, host-derived signaling molecules, and unresolved biological byproducts that arise when regulatory processes become inefficient or uncoupled.
In my recent publication in the Journal for Research in Ayurvedic sciences, I proposed a conceptual framework that attempted to explore this possibility by proposing Ama as a Gut-Derived Response Antigen Complex (GDRAC) or a Gut-Associated Molecular Complex (GAMC). These models provide an interesting systems-level approach to investigating Ama, not as a single measurable substance, but as a biologically active complex emerging from disturbed gastrointestinal regulation and host-environment interactions.
In gastrointestinal terms, this may involve a cascade of interconnected events whereby impaired digestion alters luminal contents, microbial ecology becomes dysregulated, barrier integrity is compromised, inappropriate immune activation persists, metabolic intermediates accumulate, and the host fails to adequately transform, clear, or resolve signals that would normally remain transient and self-limited.
This does not mean Ama equals endotoxin, zonulin, inflammatory cytokines, lipopolysaccharide, or any single metabolite. That would be a reductionist mistake. Rather, Ama may be studied as a systems-level pattern involving interacting intermediates generated through impaired processing, abnormal accumulation, disturbed microbial ecology, altered barrier function, and maladaptive host responses.
In non-communicable diseases, this idea becomes especially relevant because many chronic disorders do not begin as dramatic structural failures. They often emerge through low-grade, cumulative, and regulatory disturbances involving diet, metabolism, microbiota, immunity, stress, sleep, and environmental exposures.
Ama may therefore be conceptualized as a dysregulated interactome and secretome that reflects impaired transformation, inappropriate accumulation, defective clearance, and disturbed biological communication across multiple physiological networks. In this sense, Ama reflects not merely what has accumulated, but the loss of regulatory competence that allowed such accumulation to persist.
Strotas as Flow, Exchange, and Communication
The concept of Strotas offers one of the strongest bridges between Ayurveda and network physiology. Strotas is often described as channels, but in a systems biology context, it can be understood more broadly as the pathways through which movement, exchange, communication, and regulation occur.
In the gastrointestinal system, flow is not limited to food moving through the lumen. There is flow of bile, enzymes, mucus, electrolytes, immune signals, microbial metabolites, neural impulses, vascular nutrients, lymphatic drainage, and endocrine messages. These flows connect the gut to the liver, pancreas, brain, immune system, adipose tissue, and systemic metabolism.
When flow is appropriate, physiology remains coordinated. When flow is obstructed, excessive, deficient, misdirected, or poorly regulated, symptoms and disease patterns emerge.
This interpretation makes Strotas highly relevant to modern gastroenterology. Chronic constipation, diarrhea, bile acid malabsorption, reflux, dysmotility, lymphatic congestion, altered permeability, and disturbed gut-liver communication can all be viewed as disorders involving flow, exchange, and communication.
Strotas allows us to think of physiology as movement, exchange, and communication.
Koshtha as Motility and Response Phenotype
Koshtha is a particularly important concept for Integrative gastroenterology because it speaks directly about bowel habits, motility tendency, digestive response, and individual variability. It recognizes that people differ in how their gastrointestinal system responds to food, stress, environment, medicines, and routine.
In modern terms, Koshtha can be explored as a motility and response phenotype. Some individuals tend toward slow transit, heaviness, constipation, and delayed evacuation. Others tend toward rapid transit, loose stools, sensitivity, urgency, or variable bowel patterns. Some show remarkable stability, while others shift easily with diet, sleep, travel, stress, or infection.
This has clear relevance to disorders of gut-brain interaction, irritable bowel syndrome, chronic constipation, functional diarrhea, dyspepsia, reflux phenotypes, and motility disorders. It also connects to emerging tools that measure physiology more directly, including transit studies, electrogastrography, water load satiety testing, anorectal physiology, breath tests, bile acid assessment, and microbiome-metabolite profiling.
Koshtha should not be reduced to a simplistic label. It can be developed as a clinically meaningful phenotype that integrates bowel pattern, motility behavior, visceral sensitivity, diet response, and longitudinal variability.
Dosha as Regulatory Pattern
Dosha is perhaps the most widely recognized Ayurvedic concept, but also one of the most easily misunderstood. In a serious Ayurveda Biology framework, Dosha should not be treated as a fixed personality type or a superficial classification. It is more useful to interpret Dosha as a regulatory pattern that reflects tendencies in movement, transformation, stability, reactivity, and resilience.
In this context, Vata may be explored in relation to coordination, motility, neural regulation, variability, and rhythm. Pitta may be explored in relation to transformation, enzymatic activity, metabolic intensity, acid-bile physiology, and inflammatory tone. Kapha may be explored in relation to structure, lubrication, mucosal stability, anabolic tendency, and resilience.
We should never tend to view them as one to one equivalences. Vata is not simply motility, Pitta is not simply acid, and Kapha is not simply mucus. Such reductions have the potential to weaken the framework. The more useful approach is to study Dosha as a pattern language that may help organize complex physiological tendencies across multiple systems.
This is where Ayurveda Biology must be rigorous. It should not claim equivalence prematurely. It should generate hypotheses, define measurable domains, and test whether classical pattern recognition can be correlated with physiological, biochemical, microbial, metabolic, and clinical signatures.
Shatkriyakala as Disease Staging
Shatkriyakala, the six-stage model of disease evolution, offers a powerful bridge to functional staging. It recognizes that disease does not appear suddenly at the point of diagnosis. It evolves through accumulation, aggravation, propagation, localization, manifestation, and complication.
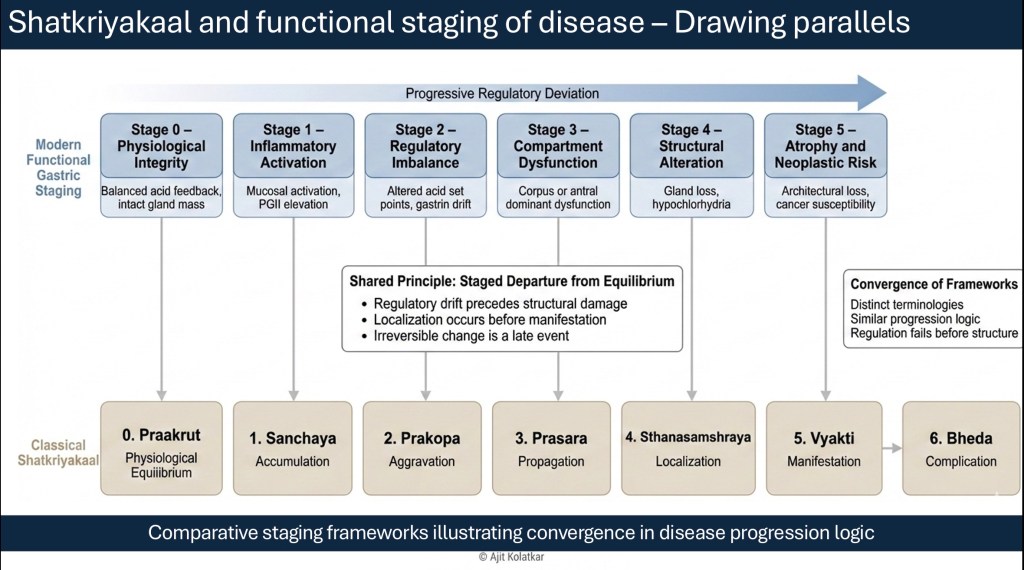
This idea is highly relevant to chronic gastrointestinal disease and non-communicable disorders. Many conditions begin with subtle dysregulation long before structural pathology becomes obvious. For eg Inflammation may precede atrophy while motility disturbance may precede visible damage likewise metabolic dysfunction may precede organ failure. Modern medicine is increasingly recognizing similar patterns through concepts such as preclinical disease, risk states, metabolic syndrome, low-grade inflammation, allostatic load, dysbiosis, barrier dysfunction, and functional staging.
Shatkriyakala can therefore be revisited as a process-based model of disease evolution. Its value lies not in replacing histology, imaging, or molecular diagnostics, but in encouraging us to ask where the patient is along a continuum of dysfunction and whether intervention can occur before structural decline becomes established.
Why This Matters for Gastroenterology
Gastroenterology is one of the most appropriate fields for developing Ayurveda Biology because the gut is where food, microbes, metabolism, immunity, sensation, motility, and behavior converge.
Dyspepsia and Gastroparesis are part of the same disease spectrum and reflux is not only acid dysfunction but rather is a resultant of disordered gastric motility apart from an LES dysfunction. Similarly it would be wrong to consider IBS as just a bowel habit. Chronic diarrhea has much more to it than infection while constipation is not only slow stool movement.
A normal endoscopy does not always mean normal GI system.
These conditions often involve layered disturbances across motility, secretion, sensation, microbial ecology, immune tone, barrier function, neuroendocrine signaling, diet response, and psychological stress. This is precisely the kind of complexity that requires a systems framework.
Ayurveda Biology can help organize and reinterprete this complexity by offering a process-based language that can be mapped carefully to modern physiological domains without reducing one system into the other.
Toward Integrative Precision Gastroenterology
The future of gastroenterology will likely require a deeper integration of structural diagnosis, physiological testing, biomarker interpretation, microbiome-metabolite analysis, diet and lifestyle assessment, and longitudinal pattern recognition.
This is where an Ayurveda Biology framework can become clinically meaningful. It can support the development of biomarker matrices, physiology-first diagnostic pathways, explainable AI models, and personalized interventions that integrate diet, behavior, pharmacology, microbiome modulation, and traditional therapeutic principles.
In such a framework, GI biomarkers like GastroPanel, fecal calprotectin, Zonulin, Defensins, iFABP, C4, fecal bile acids, pancreating function testing, breath VOC testing, electrogastrography, microbiome profiles, metabolic markers, inflammatory signals, and clinical phenotypes can be interpreted not as isolated tests, but as pieces of a regulatory map.
This is not about mixing systems casually. It is about building a disciplined translational science.
The Need for a Structured Ayurveda Biology Curriculum
If Ayurveda Biology is to evolve beyond an intellectual exercise and become a meaningful contributor to healthcare, research, and policy, it must be supported by a structured educational ecosystem. One of the major challenges in contemporary healthcare education is that disciplines continue to be taught largely in isolation. Physiology is separated from systems science, molecular biology from clinical practice, and traditional knowledge from modern research methodology. Yet the diseases that increasingly dominate global healthcare do not respect these boundaries.
Non-communicable diseases such as obesity, diabetes, metabolic syndrome, gastrointestinal disorders, autoimmune diseases, neuroinflammatory conditions, and lifestyle-related chronic illnesses rarely arise from a single cause or a single organ. They emerge from complex interactions between diet, microbiome, immunity, metabolism, stress, sleep, genetics, environment, behavior, and social context. Understanding such complexity requires a new generation of clinicians and researchers who are comfortable moving across disciplinary boundaries.
This is where Ayurveda Biology becomes particularly relevant. A rigorous Ayurveda Biology curriculum should train students to move fluently between classical Ayurvedic concepts, modern physiology, systems biology, biomarkers, computational thinking, clinical epidemiology, artificial intelligence, and translational research methods. The objective is not merely to preserve traditional knowledge, nor simply to reinterpret it through a biomedical lens, but to create scholars capable of generating new scientific questions and new models of healthcare.
Encouragingly, important steps in this direction have already begun. The MSc Ayurveda Biology program pioneered by The University of Trans-Disciplinary Health Sciences and Technology (TDU) represents one of the earliest attempts to create such an academic bridge. Similarly, recent efforts by NCISM to develop a dedicated MD program in Ayurveda Biology reflect a growing recognition that new educational frameworks are required if Ayurveda is to contribute meaningfully to contemporary science and healthcare.
These initiatives should be viewed not as isolated programs, but as the beginnings of a larger movement. If Ayurveda Biology is to fulfil its potential, it will require dedicated curricula, research centers, translational laboratories, interdisciplinary collaborations, and robust methodological training.
I strongly believe that Ayurveda has much to offer science, just as science has much to offer Ayurveda. “The future lies neither in preserving traditional knowledge unchanged nor in reducing it entirely to existing biomedical models. It lies in creating a generation capable of working at the interface of both, asking better questions, designing better studies, and developing more integrative approaches to some of the most complex health challenges of our time.”
A Direction Forward
Ayurveda Biology should not be positioned as an alternative to modern gastroenterology. It should be positioned as an expansion of the questions we ask, the frameworks and approaches we use to interpret complex disease.. The task ahead is not to prove that every classical concept has a direct biomedical equivalent. The task is to develop a disciplined science of translation, where concepts are respected in their original depth while being examined through contemporary methods.
This requires humility from both sides. Modern science must recognize that reductionism, while powerful, is not always sufficient to explain regulation. Traditional knowledge must be studied with rigor, clarity, and openness to refinement. If this is done well, Ayurveda Biology can become a meaningful contributor to the future of gastroenterology, systems medicine, and non-communicable disease research.
The future of medicine may depend not only on detecting disease earlier, but on understanding regulation better.

Leave a comment